Mood Disorders: Bipolar Disorder
Mood disorders, also known as affective disorders, are a group of psychiatric conditions characterized by disturbances in a person’s mood, leading to periods of intense sadness or excessively elevated mood.
Mood disorders, as we currently understand them, occur on a spectrum. When a person only experiences periods of intense sadness, we call it major depressive disorder (MDD), (also called unipolar depression or clinical depression). When a person experiences extreme mood swings or episodes that include emotional highs (mania or hypomania) and lows (depression), we call it bipolar disorder.
It is important to mention that the mood swings experienced by people with mood disorders are more severe than the normal ups and downs that most people experience. Mood disorders can significantly affect a person's quality of life and ability to function.
Symptoms of Depression
Feelings of intense sadness
Loss of interest or joy in hobbies
Indecisiveness
Feelings of guilt
Feelings of worthlessness
Feelings of Hopelessness
Lack of energy
Difficulty concentrating
Changes in sleep and appetite
Thoughts of suicide
Symptoms of Hypomania and Mania
Elevated or irritable mood
Increased energy
Decreased need for sleep
Inflated self-esteem or grandiosity
Talkativeness
Racing thoughts
Impulsivity
Recklessness
Below is an overview of the most common mood disorders
Major Depressive Disorder (MDD): Also known as clinical depression, MDD is characterized by persistent feelings of sadness, hopelessness, and a loss of interest or pleasure in activities. Other symptoms may include changes in appetite and sleep patterns, fatigue, difficulty concentrating, feelings of guilt or worthlessness, and thoughts of death or suicide.
Persistent Depressive Disorder (Dysthymia): Dysthymia is a chronic form of depression where individuals experience persistent depressive symptoms for at least two years. While the symptoms may be less severe than in MDD, they last longer and can lead to significant impairment in daily functioning.
Bipolar Disorders: Bipolar disorder involves recurring episodes of extreme mood swings, ranging from depressive lows to manic or hypomanic highs. During depressive episodes, symptoms are similar to those of major depression. Manic or hypomanic episodes are characterized by elevated mood, increased energy, impulsivity, and a decreased need for sleep.
Cyclothymic Disorder: Cyclothymic disorder is a chronic mood disorder characterized by numerous periods of depressive symptoms and hypomanic symptoms that do not meet the criteria for a major depressive episode or a manic episode. These mood fluctuations can last for at least two years in adults and one year in adolescents.
Seasonal Affective Disorder (SAD): SAD is a type of depression that typically occurs during specific seasons, most commonly in fall and winter. It is believed to be related to reduced exposure to sunlight and disrupted circadian rhythms. Symptoms include low mood, fatigue, increased sleep, weight gain, and decreased interest in activities.
Premenstrual Dysphoric Disorder (PMDD): PMDD is a severe form of premenstrual syndrome (PMS) that affects some women before their menstrual period. It is characterized by intense mood swings, irritability, depression, anxiety, and physical symptoms such as bloating and breast tenderness.
Other Specified and Unspecified Depressive Disorders: These categories include depressive disorders that do not meet the specific criteria for the above disorders but still cause distress and impairment. Examples include brief depressive disorder, recurrent brief depression, and other forms of subthreshold depression.
Bipolar Disorder
Bipolar disorder is a mental disorder that causes dramatic shifts in a person’s mood, energy levels, and ability to think clearly. Individuals with bipolar disorder experience high moods, known as mania or hypomania, and low moods, known as depression. These moods differ from the typical ups-and-downs most people experience. Individuals with bipolar disorder can also experience mixed moods, which include a combination of depressive and manic/hypomanic symptoms.
What is Mania and Hypomania?
Mania is defined as a distinct period of abnormally and persistently elevated, expansive, or irritable mood with abnormally and persistently increased goal-directed activity or energy that lasts for at least one (1) week.
Hypomania is similar to mania but is less severe. A hypomanic episode is a distinct period of abnormally and persistently elevated, expansive, or irritable mood and abnormally and persistently increased activity or energy that lasts at least (4) four consecutive days. Hypomanic episodes are typically not severe enough to cause marked impairment in social or occupational functioning or to necessitate hospitalization. If there are psychotic features (such as delusional thinking or hallucinations), the episode is, by definition, manic.
During a manic or hypomanic episode, a combination of the following symptoms is present and represents a noticeable change in behavior (see below).
Elevated or irritable mood
Increased energy
Decreased need for sleep
Inflated self-esteem or grandiosity
Talkativeness
Racing thoughts
Impulsivity
Recklessness
If drugs or medications cause the symptoms above, then we consider this a medication (or substance)-induced manic or hypomanic state. However, a full manic or hypomanic episode that emerges due to medication (e.g., antidepressants) or drugs (e.g., cocaine, amphetamines) but persists beyond the physiological effect of the medication or drug is sufficient for a diagnosis of mania or hypomania.
Bipolar Subtypes
Bipolar disorder is classified into subtypes such as bipolar I disorder and bipolar II disorder.
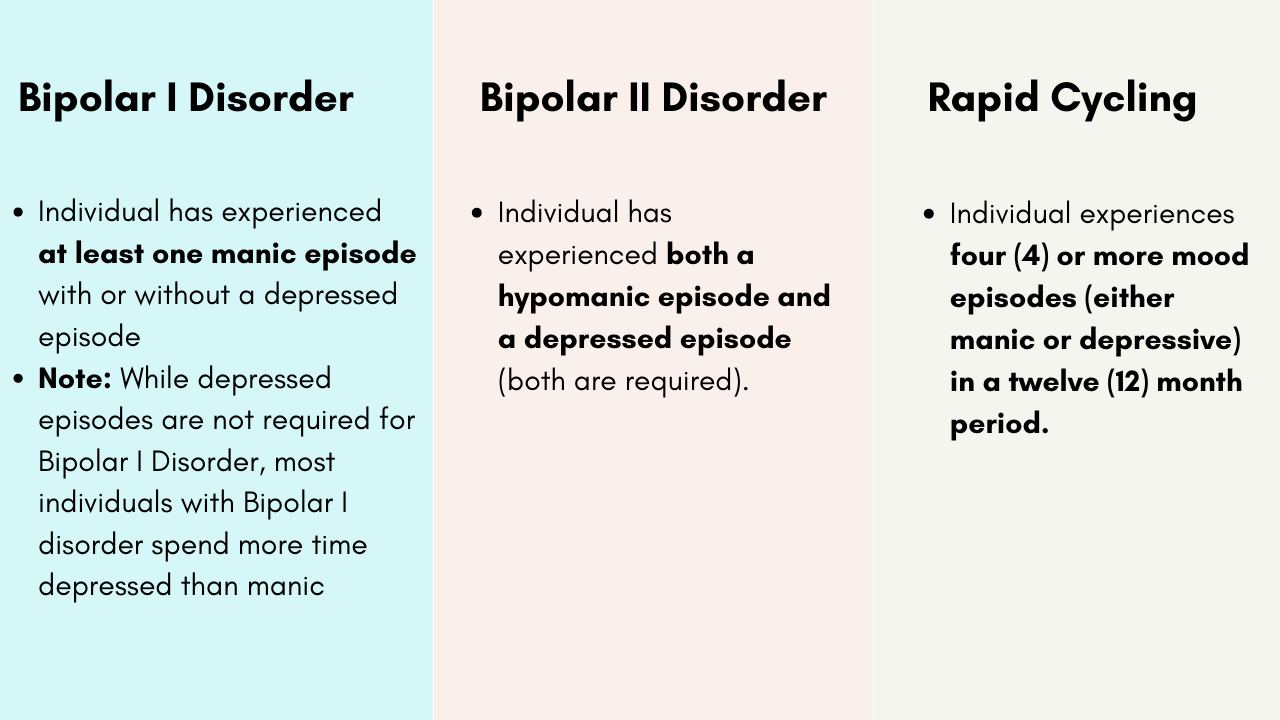
Mean age at onset of the first manic, hypomanic, or major depressive episode is approximately 18 years for bipolar I disorder and mid-20s for bipolar II disorder. Bipolar disorder most often begins with a depressive episode and is not recognized as bipolar disorder until a hypomanic or manic episode occurs; this happens in about 12% of individuals with an initial diagnosis of major depressive disorder.
Many individuals experience several episodes of major depression before experiencing a hypomanic or manic episode. Individuals with major depressive disorder, who later are diagnosed with a bipolar disorder, often have an onset of the illness in adolescence, a history of psychotic features, or a family history of bipolar illness.
Because depressed episodes often precede the first hypomanic or manic episode, many patients with bipolar disorder are initially misdiagnosed as having major depressive disorder. This is a major reason why those with bipolar disorder go undiagnosed or misdiagnosed for many years (about 10 years).
It is also worth mentioning that classic SSRI/SNRI antidepressants such as sertraline (Zoloft), Paroxetine (Paxil), Citalopram (Celexa), Fluoxetine (Prozac), Venlafaxine (Effexor), and Duloxetine (Cymbalta) may be ineffective or induce irritability, agitation, hypomania, and/or rapid cycling of moods in individuals with bipolar disorder.
Unfortunately, bipolar depression and unipolar depression are very difficult, if impossible, to differentiate. Clinical experience and some empirical evidence suggest that hypersomnia (more sleeping), apathy, increased appetite (craving for simple carbohydrates), and weight gain may be more suggestive of bipolar depression, but this is controversial.
It is also important to mention that individuals with bipolar disorder experience depressive symptoms more often than hypomanic, manic, or mixed episodes. That is, most mood episodes experienced by someone with bipolar disorder are depressive.
Rapid Cycling
Rapid cycling in bipolar disorder (BD) is a descriptor that defines a subset of patients that have a large number of episodes over short periods of time. Specifically, rapid cycling is defined as having 4 or more episodes in a 12-month period, but many patients experience more than this.
Individuals with rapid cycling generally have a younger age of onset, greater disease burden, and greater exposure to antidepressants.
Cannabis, alcohol, caffeine, steroids, selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and Tricyclic Antidepressants have been associated with inducing rapid cycling.
The Neurobiology of Bipolar Disorder
Bipolar disorder is a complex disorder. The cause of bipolar disorder is not fully understood but there are several contributing factors that include genetic influences (e.g., family history of bipolar illness), environmental influences (e.g., stress and circadian rhythm disruptions), and biochemical factors (e.g., drug abuse and hormonal imbalances). Neurophysiological changes in specific neural networks in the brain have been suggested as the primary pathophysiology of bipolar disorder.
Disrupted circadian rhythms are often harbingers of mood episodes in individuals with underlying bipolar disorder. It is unclear whether the natural course of the illness causes disturbances in sleep or disturbances in sleep precipitate mood episodes. However, it is well known that disruptions in an individual’s sleep cycle present a major risk for mood instability. This is particularly true for those with mood disorders such as bipolar disorder and major depressive disorder.
Human studies have found increased concentrations of noradrenaline (norepinephrine) and dopamine (DA) and decreased concentrations of serotonin (5-HT) in manic patients. This suggests that norepinephrine and dopamine dysregulation may play a primary role in manic symptoms. In addition to monoamine dysregulation, there is evidence implicating the glutamate and GABA systems in the pathophysiology of bipolar disorder. Animal studies suggest increased glutamatergic neurotransmission via NMDA receptors in manic patients. In addition, the efficacy of anticonvulsants, NMDA antagonists (e.g., ketamine), and benzodiazepines in the treatment of bipolar disorder suggests that glutamate and GABA systems are involved.
Circadian rhythms are consistently disturbed in patients with bipolar disorder. Researchers are investigating whether circadian rhythm disturbances might lead to mania given the fact that lithium deactivates the transcription factor GSK3B enzyme which is thought to reset the circadian clocks and restore normal brain functioning.
Functional Neuroimaging Studies have demonstrated or suggested that the following areas are implicated in bipolar disorder: prefrontal cortex, limbic areas such as the hippocampus, amygdala, anterior cingulate, and the ventral striatum (nucleus accumbens). A number of brain circuits have been implicated in the pathophysiology of bipolar disorder. Many of these circuits are involved in the regulation of emotion and cognition. Decreased activation of the orbitofrontal (OFC) circuits during a go-no go test in manic patients may explain the impulsive behaviors. Recall that the OFC is an important region within the prefrontal cortex involved in impulse-control and compulsive behaviors. The dorsolateral prefrontal cortex is involved in attentional processes and its dysfunction may also play a role in the pathophysiology of bipolar disorder. Decreased size and activity of the prefrontal cortex (PFC) has been demonstrated in patients with bipolar disorder—similar to that found in patients with unipolar depression. Interestingly, after four weeks of lithium treatment (but no valproic acid) there was an increase in gray matter volume in bipolar patients. Amygdalae are larger and more active in the bipolar patients. Bipolar disorder may be the result of abnormal interactions between the PFC and subcortical regions such as the amygdala—an abnormality not usually seen with unipolar depression. Reasons for the reduction in brain volumes and cell loss remain a mystery but could be from environmental stressors, neurodevelopmental abnormalities, and/or dysfunction in neurotransmitter systems.
Treatment of Bipolar Disorder
If left untreated, bipolar disorder usually worsens. And this highlights the importance of a good treatment plan that includes psychotherapy, mood-stabilizing medications, a healthy lifestyle, maintenance of sobriety, a consistent sleep schedule and early identification of symptoms. The management of bipolar disorder is multidimensional. The main objectives of pharmacotherapy (medication management) in bipolar disorder are to treat the acute manic/hypomanic and depressive episodes and minimize their recurrence.
Manic episodes are treated with one or more of the following: Lithium, valproate (Depakote), carbamazepine (Tegretol), lamotrigine (Lamictal), asenapine (Saphris), olanzapine (Zyprexa), risperidone (Risperdal), paliperidone (Invega), ziprasidone (Geodon), cariprazine (Vraylar), or aripiprazole (Abilify), clonazepam (Klonopin), diazepam (Valium), or lorazepam (Ativan).
Bipolar depressive episodes are treated with one or more of the following: Lithium, cariprazine (Vraylar), quetiapine (Seroquel), lurasidone (Latuda), Fluoxetine-Olanzapine combination (OFC), or lamotrigine (Lamictal).
Other disorders such as anxiety and attention deficit hyperactivity disorder should be managed as well.
Neuromodulatory modalities such as neurofeedback, Transcranial Magnetic Stimulation (TMS), and ketamine infusion therapy should be considered if medication and therapy are not effective (or only partially effective).
While medication, neuromodulatory modalities, and drug abstinence are important in the management of bipolar disorder, they are considered components of a comprehensive treatment plan. As such, individual and/or family psychotherapy and psychoeducation should be incorporated.
Bipolar Depression

Bipolar Mania and Mixed States

Bipolar Maintenance (preventing mood episodes)

Observational studies suggest that with each mood episode the time between episodes shortens. This highlights the importance of relapse prevention, which may improve long-term prognosis.
For preventing manic episodes, the following medications are preferred: Lithium, Aripiprazole (Abilify), Quetiapine (Seroquel), Olanzapine (Zyprexa), and Valproic Acid (Depakote).
For preventing depressive episodes, the following medications are preferred: Quetiapine (Seroquel), Lamotrigine (Lamictal), Lithium, and Lurasidone (Latuda).
It is important to remember that the management of neuropsychiatric disorders is multifactorial, and medication is only one component.
Bipolar Depression vs. Unipolar Depression
Distinguishing between unipolar depression and the depressive phase of bipolar disorder is crucial for several reasons, mainly related to treatment, prognosis, and managing the course of the illness. A wrong diagnosis can lead to inappropriate treatment, which might result in more mood instability.
Unipolar depression is typically treated with antidepressant medications, psychotherapy, or a combination of both. On the other hand, bipolar depression requires a different medication approach, which may include mood stabilizers (such as lithium or valproic acid), antipsychotic medications, and sometimes antidepressants in conjunction with mood stabilizers or antipsychotics to prevent triggering a manic episode.
Treating bipolar depression as if it was unipolar depression can be dangerous. For instance, prescribing classic antidepressants to someone with bipolar depression can potentially worsen the depression or trigger a manic or hypomanic episode, known as "switching.” Irritability, agitation, psychosis, and rapid cycling of moods may also occur if bipolar depression is treated as if it was unipolar depression.
Unfortunately, the depressive phase of bipolar disorder is nearly identical to the unipolar depression. This is why it is important to report any history of manic or hypomanic episodes as most people with bipolar disorder experience the depressive phase prior to their first hypomanic or manic episode.
Although both conditions are chronic and recurrent, their courses can be quite different. Bipolar disorder involves cycling between depressive and manic (or hypomanic) states, which has different implications for long-term management and treatment strategies. Monitoring for symptoms of hypomania and mania is crucial for developing an effective treatment plan.
BIPOLAR DISORDER DIAGNOSIS AND TREATMENT GUIDELINES (PDF)
Helping Someone with Bipolar Disorder - HelpGuide.org
For more information about Depression, click here.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC.
Arciniegas, Yudofsky, Hales (editors). The American Psychiatric Association Publishing Textbook Of Neuropsychiatry And Clinical Neurosciences. Sixth Edition.
Bear, Mark F.,, Barry W. Connors, and Michael A. Paradiso. Neuroscience: Exploring the Brain. Fourth edition. Philadelphia: Wolters Kluwer, 2016.
Charney DS. Monoamine dysfunction and the pathophysiology and treatment of depression. Journal of Clinical Psychiatry. 1998;59(Suppl):11–14.
Cooper, J. R., Bloom, F. E., & Roth, R. H. (2003). The biochemical basis of neuropharmacology (8th ed.). New York, NY, US: Oxford University Press.
Higgins, E. S., & George, M. S. (2019). The neuroscience of clinical psychiatry: the pathophysiology of behavior and mental illness. Philadelphia: Wolters Kluwer.
Hillhouse, T. M., & Porter, J. H. (2015). A brief history of the development of antidepressant drugs: from monoamines to glutamate. Experimental and clinical psychopharmacology, 23(1), 1–21. doi:10.1037/a0038550
Iversen, L. L., Iversen, S. D., Bloom, F. E., & Roth, R. H. (2009). Introduction to neuropsychopharmacology. Oxford: Oxford University Press.
Mendez, M. F., Clark, D. L., Boutros, N. N. (2018). The Brain and Behavior: An Introduction to Behavioral Neuroanatomy. United States: Cambridge University Press.
Papakostas GI, Thase ME, Fava M, Nelson JC, Shelton RC. Are antidepressant drugs that combine serotonergic and noradrenergic mechanisms of action more effective than the selective serotonin reuptake inhibitors in treating major depressive disorder? A meta-analysis of studies of newer agents. Biological Psychiatry. 2007.
Papakostas GI. Serotonin norepinephrine reuptake inhibitors: Spectrum of efficacy in major depressive disorder. Primary Psychiatry. 2009;16(Suppl 4):16–24.
Schatzberg, A. F., & DeBattista, C. (2015). Manual of clinical psychopharmacology. Washington, DC: American Psychiatric Publishing.
Schatzberg, A. F., & Nemeroff, C. B. (2017). The American Psychiatric Association Publishing textbook of psychopharmacology. Arlington, VA: American Psychiatric Association Publishing.
Neuroscience, Sixth Edition. Dale Purves, George J. Augustine, David Fitzpatrick, William C. Hall, Anthony-Samuel LaMantia, Richard D. Mooney, Michael L. Platt, and Leonard E. White. Oxford University Press. 2018.
Stahl, S. M. (2013). Stahl's essential psychopharmacology: Neuroscientific basis and practical applications (4th ed.). New York, NY, US: Cambridge University Press.
Hales et al. The American Psychiatric Association Publishing Textbook of Psychiatry. 6th Edition.
Benjamin J. Sadock, Virginia A. Sadock. Kaplan & Sadock's Comprehensive Textbook of Psychiatry. Tenth Edition. Philadelphia. Wolters Kluwer. 2017.
_____
This post was reviewed by a medical professional.